Arterial Switch Operation - Background
In transposition of the great arteries (see Fig. 1), the aorta arises from the right ventricle and the pulmonary artery from the left ventricle. 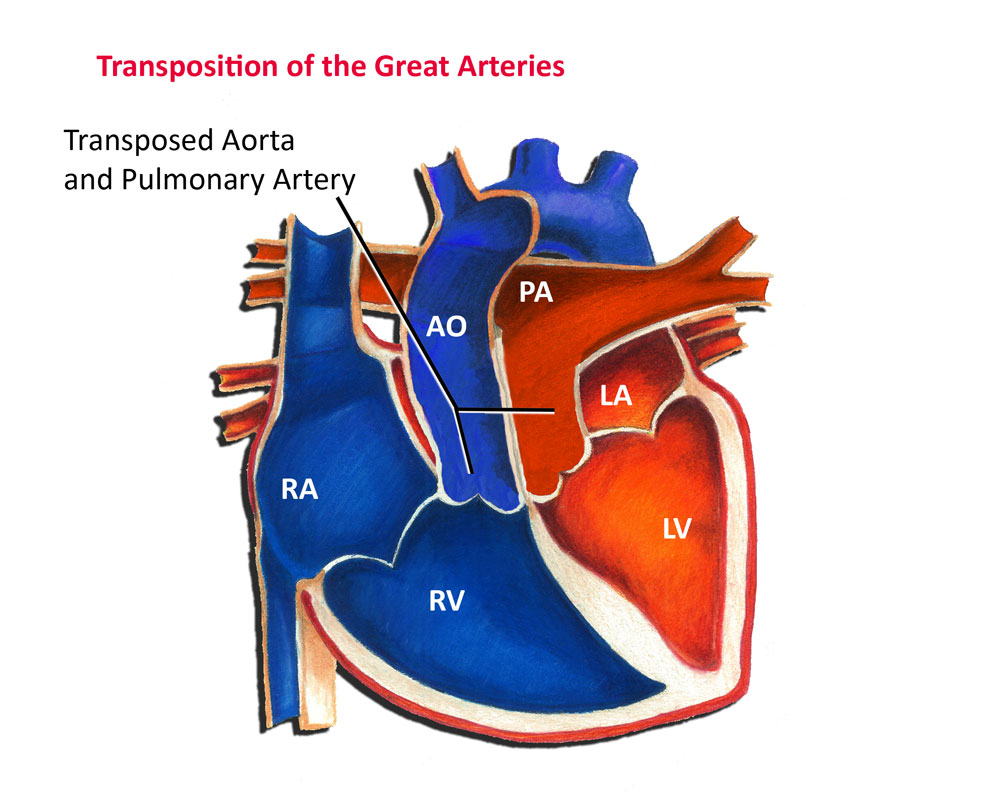 Deoxygenated, or blue blood, returning from the body is sent directly back out to the body again. Likewise, oxygenated, or red blood returning from the lungs is sent right back out to the lungs. Mixing is only possible if there is an atrial septal defect and/or a patent ductus arteriosus. In the absence of successful mixing, transposition of the great arteries is usually fatal.
Deoxygenated, or blue blood, returning from the body is sent directly back out to the body again. Likewise, oxygenated, or red blood returning from the lungs is sent right back out to the lungs. Mixing is only possible if there is an atrial septal defect and/or a patent ductus arteriosus. In the absence of successful mixing, transposition of the great arteries is usually fatal.
There have been a number of different surgical approaches to repairing transposition of the great arteries over the years. The arterial switch operation was actually first tried in the 1950s by Dr. William Mustard. Unfortunately his initial attempts were unsuccessful and the technique was largely abandoned in favor of the Senning and later Mustard procedures. These procedures were not true "anatomical correction" of transposition of the great arteries, but rather simply served to reroute systemic and pulmonary venous blood flow to the appropriate ventricles.
The arterial switch operation was first successfully performed in 1975 by Dr. Adib Jatene. Over the years the surgical techniques of the arterial switch operation have been refined and improved to the point that it is a fairly safe operation in this day and age.
Arterial Switch Operation - Details
As shown in the figures below, the initial step (Step 1) in the operation involves transecting or cutting through both the aorta and pulmonary artery while the patient is on cardiopulmonary bypass. The coronary arteries are then removed from the aortic root and transferred to the pulmonary root, which will become the "new" aorta (Step 2). The main pulmonary artery is brought forward, and then both the pulmonary artery and aorta are reattached to their new respective locations (Step 3).
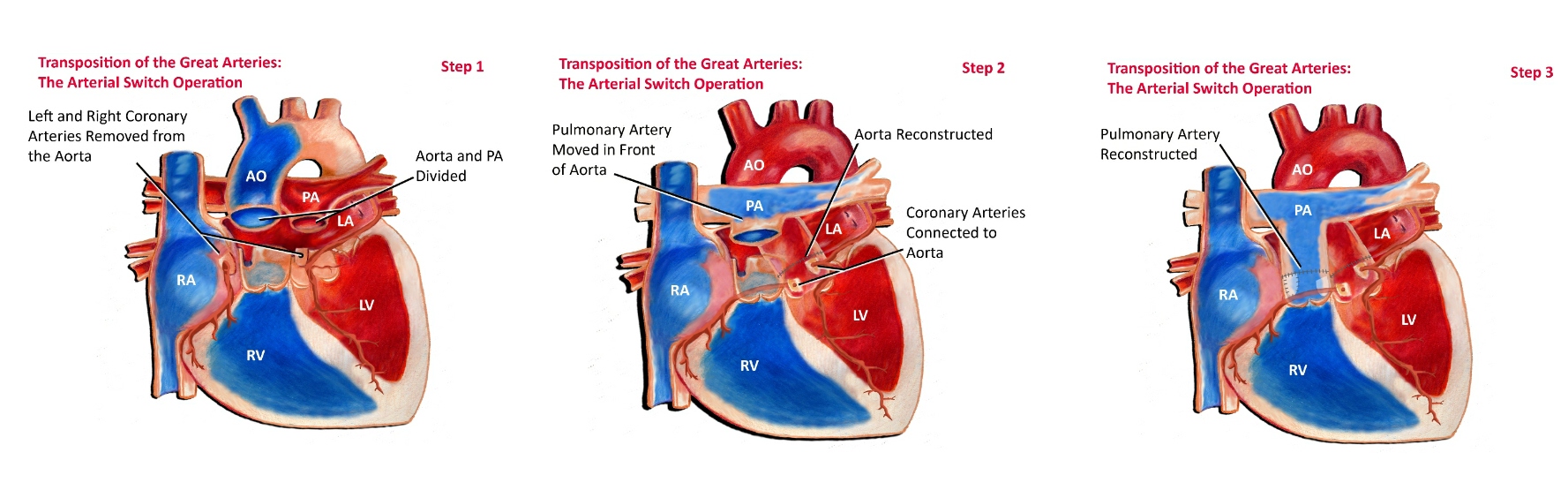
Technically the most challenging aspect of the surgery is transferring with the coronary arteries. The size of a baby's heart is not much bigger than its fist. Accordingly, it is easy to appreciate how small and delicate the coronary arteries are. The coronary arteries play an extremely important role in providing blood flow to the heart. Any injury or even minor distortion of the coronary arteries can be devastating. Great care must be taken to allow for proper localization and repositioning of both coronary arteries.
On occasion, pre-existing coronary artery anomalies may complicate the arterial switch operation. In some instances a branch of the normal left coronary artery is found arising from the right coronary artery. In other instances part of the coronary artery may actually run inside the wall of the aorta. In this situation the coronary artery can still be successfully transferred, however this finding can increase the challenges and risk involved.
Associated heart defects may increase the complexity of the surgery as well. Most patients with transposition of the great arteries have an accompanying atrial septal defect and patent ductus arteriosus. These are usually addressed at the time of surgery as well. In some instances there may be a ventricular septal defect which needs to be closed. Some patients have the presence of pulmonary valve stenosis, or even narrowing below the pulmonary valve. This may complicate things considerably, and in some instances require a different surgical approach altogether. Finally, some patients may have an associated coarctation of the aorta. This can also complicate the surgery.
Fortunately in this day and age the outcomes for a child undergoing an arterial switch operation are generally very good. The majority of children do fine and end up leading normal, healthy lives.