Tetralogy of Fallot is a cyanotic heart defect consisting of a ventricular septal defect, pulmonary valve stenosis, and varying degrees of aortic override and right ventricular hypertrophy. It is most common cyanotic congenital heart defect in children. In the absence of any symptoms or significant cyanosis, surgery for tetralogy of Fallot is usually performed sometime in the first year of life. Often allowing a baby to grow for several months can make the surgery technically easier and allow for a better outcome.
Tetralogy of Fallot Surgery: Blalock-Taussig Shunt
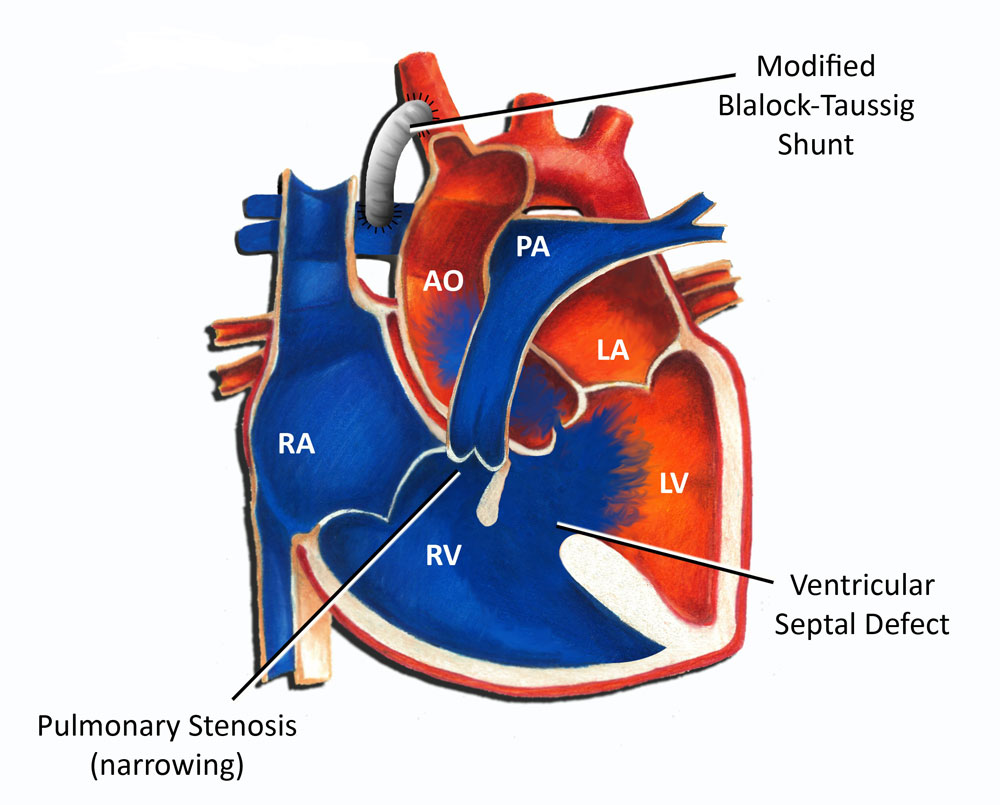
In children who are born with significant cyanosis, intervention is usually needed early on, often in the first week of life. Usually this takes the form of a Blalock Taussig shunt (BT shunt). Originally performed by Drs. Blalock and Taussig in Baltimore in 1944, a shunt is simply a connection between the systemic circulation and the pulmonary circulation (see illustration below). A shunt allows for blood to gain access to the lungs in order to obtain oxygen. Originally shunts were performed using a child's native blood vessels (classic BT shunt); in this day and age they are performed using artificial material (modified BT shunt).
Tetralogy of Fallot Surgery: Complete Repair
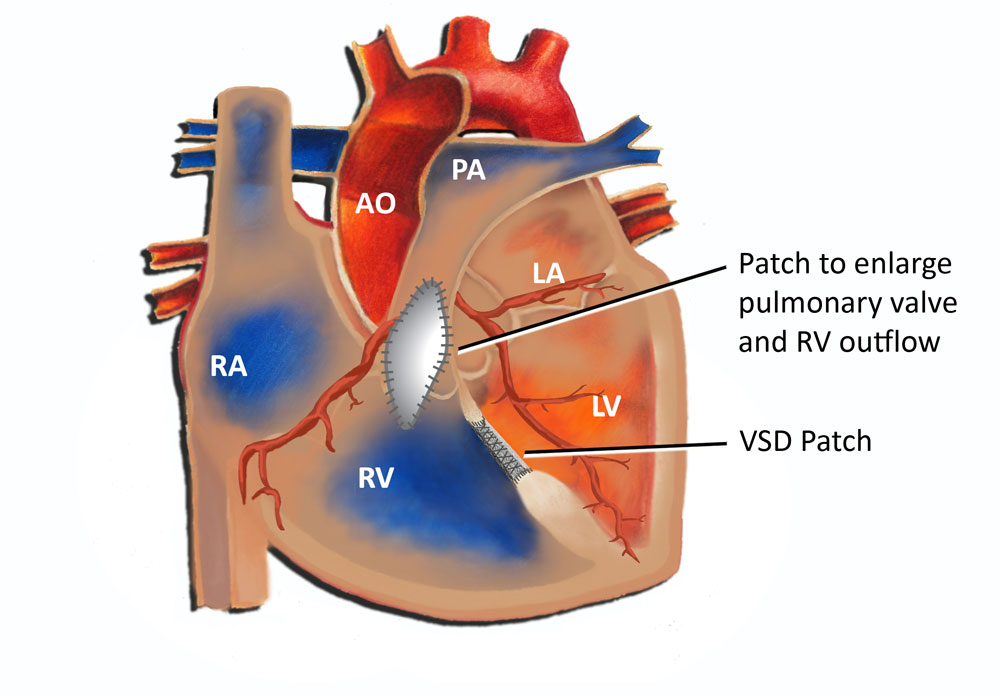
Complete surgical repair of tetralogy of Fallot involves closing the ventricular septal defect and widening the outflow to the lungs. This can take the form of removing muscle in the right ventricle beneath the pulmonary valve, incising and opening the pulmonary valve, and frequently cutting across the ring which the valve sits on, called the pulmonary valve annulus (see illustration below). Inevitably in most cases this leads to some degree of leakage of the pulmonary valve. The vast majority of children following surgery for tetralogy of Fallot develop some degree pulmonary valve insufficiency or leakage. Although this does not cause an immediate problem, it can become an issue over time.
In the absence of significant complicating features, the vast majority of children in this this day and age who undergo tetralogy of Fallot repair do very well. Most older infants require hospitalization between 4-7 days and usually have recovered nicely by the time they are discharged. All children who undergo heart surgery are required to take antibiotics before any dental or surgical procedures for at least 6 months following surgery (SBE prophylaxis). The manipulation of the heart and the presence of synthetic tissue in the heart increases the risk of infection at any time bacteria may enter the bloodstream. This can happen with dental work and certain forms of surgery. After 6 months, usually the normal heart tissue has sealed things in place sufficiently to no longer require this.
The long-term prognosis of children who undergo tetralogy of Fallot surgery is very good. A portion of children with long-standing pulmonary valve regurgitation will ultimately require replacement of the pulmonary valve, usually as teenagers or young adults. Even with this, however, the majority do very well with normal development and little if any limitations.